Book Appointment Now
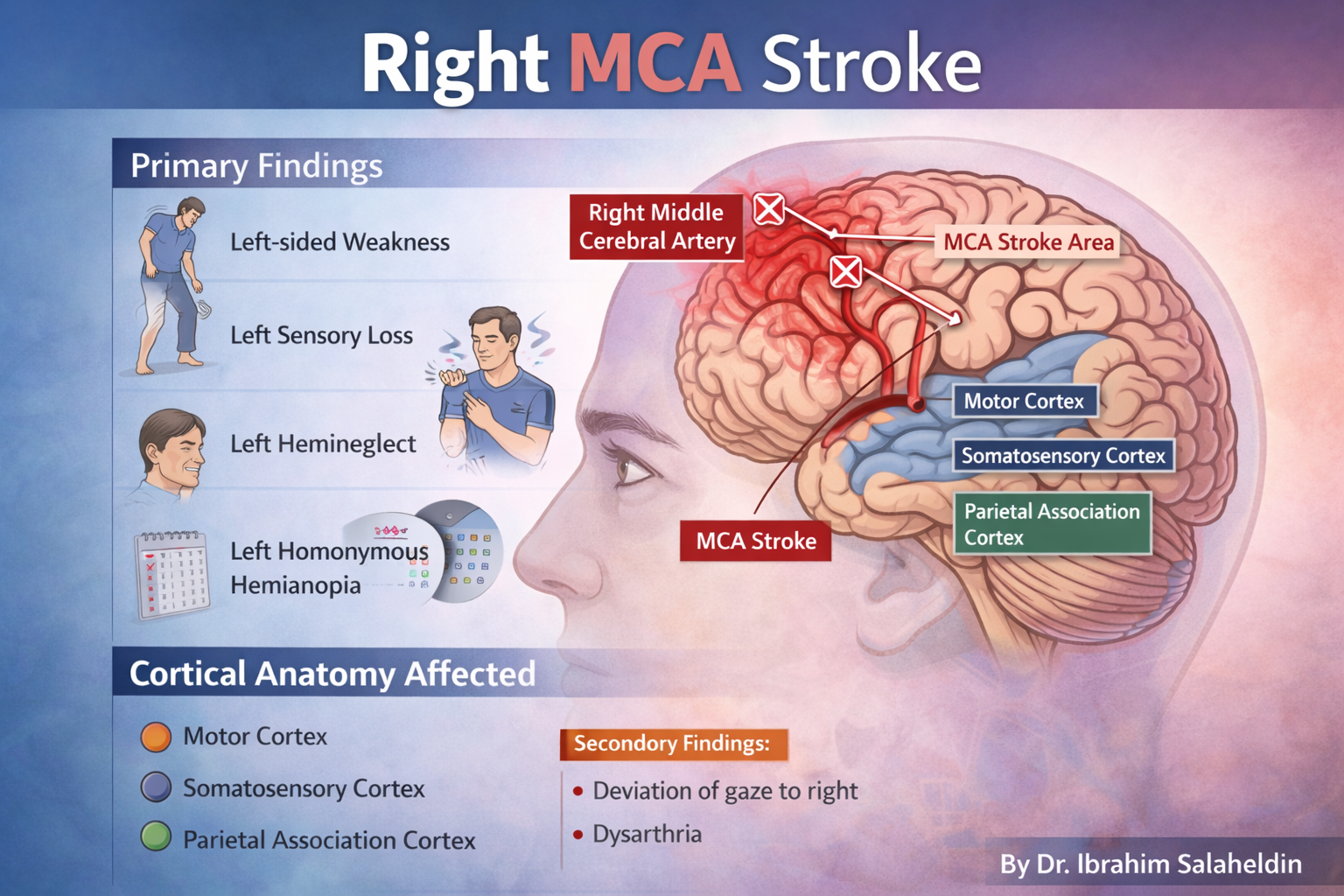
Right Middle Cerebral Artery (MCA) Stroke
Author: Dr Ibrahim Elpum
Introduction
Right Middle Cerebral Artery (MCA) stroke is one of the most frequently tested cerebrovascular syndromes in MRCP, USMLE, and medical school examinations. It produces a characteristic clinical pattern that becomes straightforward to recognise once the principles of cortical localisation and functional neuroanatomy are understood. This guide emphasises conceptual understanding to help candidates approach exam questions with confidence rather than relying on memorisation.
Vascular Anatomy (Concept First)
The Middle Cerebral Artery (MCA) is the largest branch of the internal carotid artery and supplies:
- Lateral surface of frontal, parietal, and temporal lobes
- Primary motor cortex (face and upper limb area)
- Primary sensory cortex (face and upper limb area)
- Frontal eye field
- Parietal association cortex (attention and spatial awareness)
- Optic radiation (Meyer’s loop and superior fibres)
- Dominant hemisphere language areas (Broca’s and Wernicke’s) — if left MCA
A right MCA stroke therefore mainly affects:
Motor, sensory, visual, and attentional functions of the left side of the body
Core Clinical Pattern
Right MCA stroke classically produces:
Left-sided weakness + left sensory loss + left visual field defect + left neglect
This pattern reflects damage to:
- Motor cortex → weakness
- Sensory cortex → sensory loss
- Optic radiation → homonymous hemianopia
- Right parietal lobe → hemispatial neglect
Motor Features
Left face and arm weakness > leg weakness
→ Involvement of the lateral primary motor cortex
The homunculus explains the pattern:
- Face and upper limb areas lie on the lateral cortex (MCA territory)
- Leg area lies medially (ACA territory)
So MCA strokes typically cause:
Arm and face more affected than the leg
Sensory Features
Left-sided sensory loss (face and arm > leg)
→ Involvement of the primary somatosensory cortex
Patients may describe:
- Numbness
- Reduced pinprick sensation
- Impaired proprioception on the left side
Visual Features
Left homonymous hemianopia
→ Involvement of optic radiation in the temporal and parietal lobes
This leads to:
- Loss of the left visual field in both eyes
- Patients bumping into objects on their left
The Hallmark of Right MCA Stroke: Neglect
Left hemispatial neglect
→ Involvement of the right parietal association cortex
This is one of the most high-yield exam features.
Patients may:
- Ignore the left side of their body
- Eat only from the right side of the plate
- Draw only half of a clock
- Shave only the right side of their face
Exam pearl:
Neglect is classically a feature of right hemisphere lesions (not left).
Eye Findings
Gaze deviation towards the right
→ Involvement of the right frontal eye field
The eyes are “pulled” towards the side of the lesion:
Right MCA stroke → eyes deviate to the right
Speech and Language
In a right MCA stroke:
- Language is usually preserved (in most right-handed people)
Language deficits occur mainly with:
Left MCA stroke (dominant hemisphere)
This distinction is commonly tested in exams.
Common Exam Trap: Right vs Left MCA
| Feature | Right MCA | Left MCA |
|---|---|---|
| Contralateral weakness | Left | Right |
| Contralateral sensory loss | Left | Right |
| Homonymous hemianopia | Left | Right |
| Hemispatial neglect | Yes (classic) | Rare |
| Aphasia | No | Yes |
One-line exam pearl:
Neglect = Right parietal lobe = Right MCA stroke.
How to Visualise It Clinically
Imagine a patient with a right-sided cortical stroke:
- Face droops on the left
- Left arm weak an